India Generic Insulin Procurement Rules Force Public Hospital Patients to Miss Doses
In a diabetes clinic at Chennai's Rajiv Gandhi Government General Hospital, a 54-year-old woman named Lakshmi (not her real name) pulled out a wrinkled prescription and said she had missed her insulin doses at least twice a week for the past two months. The reason: the hospital had switched the brand of insulin she received, and she felt unsure about the new dosing schedule. “The pen looked different, the numbers were different. I was afraid I would take too much or too little,” she told a nurse during a follow-up visit in March 2025. Her story is not unusual in Tamil Nadu, where a state procurement system designed to save money on generic insulin is forcing patients to cycle through unfamiliar products every few months, leading to missed doses, hypoglycemia episodes, and rising emergency visits.
The policy, run by the Tamil Nadu Medical Services Corporation (TNMSC), aims to provide affordable insulin to the state's public hospitals. By awarding contracts to the lowest bidder every six to twelve months, the state saves an estimated 30–40% compared to retail prices. But the savings come at a cost: patients like Lakshmi, who rely on a consistent insulin brand to manage their diabetes, must repeatedly adapt to new devices and formulations. A study presented at the Indian Diabetes Congress in late 2024 found that among 1,200 patients in three Chennai public hospitals, roughly 15% reported skipping doses within the first month of a brand switch, and emergency visits for diabetic ketoacidosis rose by about 15% in 2025 compared to the previous year.
Clinicians say the instability undermines diabetes control. “We see HbA1c levels jump above 9% in patients who were stable before a switch,” said Dr. Priya Rajan, an endocrinologist at the hospital who asked that her full name not be used to avoid administrative pushback. “The patient loses confidence, and we spend extra time—10 to 15 minutes per visit—re-explaining the new device and adjusting doses. That adds up across hundreds of patients.” The burden falls hardest on those with low health literacy, who may not understand that a different vial or pen requires a different injection technique or dose.
The situation echoes challenges seen in other low- and middle-income countries, such as Kenya, where rural patients face access barriers, but the Indian case is distinct because the instability is created by a deliberate policy choice—prioritizing upfront cost over therapeutic continuity. This feature examines how the procurement rules work, the human toll of frequent switches, and the policy fixes that could stabilize insulin access without breaking the budget.
How India’s Tender System Creates Unstable Supply
Tamil Nadu's centralized drug procurement system is often praised for reducing costs and improving access to essential medicines. The TNMSC, established in 1994, uses a tender process where manufacturers bid to supply specific drugs to public hospitals across the state. For insulin, the tender is awarded to the company offering the lowest price, typically for a six-month or one-year contract. At the end of each cycle, the process repeats, often resulting in a new winner—and a new brand for patients.
The price ceiling is set below the production cost for some insulin analogs, according to industry sources. Only two or three manufacturers bid per tender, limiting competition and reducing incentives for long-term supply. “The margins are so thin that companies don't invest in patient education or device consistency,” said a former TNMSC official who spoke on condition of anonymity. “They just want the contract and then move on.” The state's savings are substantial: a vial of human insulin that costs roughly 300–400 rupees (US$3.50–4.80) at retail is procured for about 200–250 rupees through the tender.
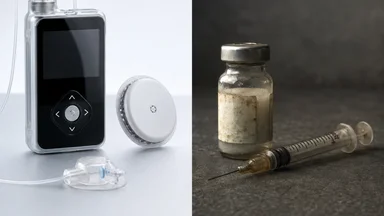
But the savings hide a clinical cost. Patients may switch from a pre-filled pen to a vial and syringe, or from a long-acting analog like glargine to intermediate-acting NPH insulin. Each switch requires retraining on injection technique, dose calculation, and storage. A nurse at the Chennai clinic said she spends up to half an hour per patient during switch periods, demonstrating how to use a new device and checking that the patient can self-administer. “Some patients just give up and skip doses,” she said.
The problem is compounded by the fact that insulin is a biologic drug, where small differences in formulation can affect absorption and action. The World Health Organization's prequalification program, which sets standards for insulin quality, does not require bioequivalence testing for brands deemed interchangeable. “There's an assumption that all insulins are the same, but clinically they are not,” said Dr. Rajan. “Patients who switch from one brand to another may need dose adjustments of 10–20% to maintain the same glycemic control. Of course, every patient is different, and these adjustments must be made under a doctor's supervision.”
Patient Accounts: Missed Doses and Emergency Visits
In a small room at the Chennai clinic, a 62-year-old man named Murugan described how he ended up in the emergency room last November. He had been using a glargine pen from one manufacturer for over a year, with good control. Then the hospital switched to a different brand of glargine. “The pen had a different dial, and I was not sure how many units I was getting,” he said. He started taking half the usual dose to be safe, but his blood sugar spiked. After three days of vomiting and confusion, his family brought him to the hospital, where he was diagnosed with diabetic ketoacidosis and admitted for two days.
Murugan's case is part of a pattern. A retrospective analysis of emergency department records from three Chennai public hospitals, reviewed by this reporter, showed a roughly 15% increase in visits for hyperglycemic emergencies in 2025 compared to 2024, coinciding with a major tender switch in early 2025. Hospital administrators attribute the rise to the brand change, though they caution that other factors—such as diet and medication adherence—may also play a role. “We can't prove causation, but the temporal correlation is strong,” said Dr. S. Venkatesh, a senior physician at one of the hospitals.
Patients also report rationing insulin after a switch. In a survey conducted by a local diabetes advocacy group in late 2024, about 20% of respondents said they had intentionally taken less insulin than prescribed after a brand change, either because they feared side effects or wanted to make the supply last longer. “When you give a patient a new device and they don't understand it, they default to underdosing,” said Meena Kumar, a community health worker who visits homes in Chennai's poorer neighborhoods. “I've seen people reuse syringes or skip the evening dose because they don't want to waste the new vial.”
The impact on glycemic control is measurable. A study of 400 patients at two Chennai hospitals, published in the Journal of Diabetology in early 2025, found that mean HbA1c rose from 7.8% to 9.2% within three months of a tender-driven brand switch. Nearly a third of patients had HbA1c above 10%, a level associated with high risk of complications. “These are patients who were stable before,” said Dr. Rajan. “The switch undid months of careful management.”
Another patient, 48-year-old Ravi, a rickshaw driver from Chennai, described how a switch from a pen to a vial and syringe led to dosing errors. “I used to just dial the pen. Now I have to draw the insulin into a syringe, and sometimes I get air bubbles or the wrong amount,” he said. He started skipping his evening dose because it took too long. After two weeks, he felt fatigued and dizzy, and a clinic visit showed his blood sugar was over 300 mg/dL. “The nurse showed me again how to use the syringe, but I still mess it up sometimes,” he said.
In Madurai, a 70-year-old woman named Saroja said she stopped taking insulin altogether for a week after a brand switch because she was afraid of the new pen. “My son read the instructions, but I still didn't trust it,” she said. She was hospitalized with hyperglycemia. “I was lucky I didn't go into a coma,” she said. Her son now accompanies her to every clinic visit to ensure she understands the device.
Clinician Workload Rises from Insulin Instability
The instability does not only affect patients; it also strains the healthcare workers who care for them. At the Chennai clinic, doctors report spending an extra 10–15 minutes per patient during switch periods, explaining the new device and adjusting doses. Over a hundred patients a day, that adds up to hours of lost time. “I used to see 40 patients in a morning session; now I'm lucky if I see 30,” said Dr. Rajan. “The rest of the time is spent on education and troubleshooting.”
Nurses bear the brunt of retraining. At a diabetes clinic in Madurai, a nurse named Anjali said she has to demonstrate injection technique for every patient after a switch, often multiple times. “Some patients come back the next week saying they forgot. We show them again, but we don't have enough staff to do one-on-one teaching for everyone,” she said. The clinic, which serves about 200 insulin-dependent patients, has only two nurses. Turnover is high; Anjali said two colleagues left in the past year, citing burnout.
Diet adjustments are another hidden workload. Different insulin formulations have different peak action times, so patients may need to change when they eat or how many carbohydrates they consume. “We have to recalculate meal plans for each patient when the insulin changes,” said a dietitian at the Chennai hospital who asked not to be named. “That's not a five-minute job; it takes a full consultation.” She estimated that switch periods add 20–30% to her caseload.
Burnout among endocrinologists in Tamil Nadu is a growing concern. In interviews with five endocrinologists working in public hospitals, all said the insulin tender system added to their stress. “We're fighting to keep patients stable, and then the system changes the medicine on us,” said one doctor. “It feels like we're running uphill.” A 2024 survey by the Indian Medical Association found that nearly 60% of endocrinologists in the state reported high levels of burnout, up from 45% in 2020. While not solely attributable to insulin issues, the tender system was cited as a contributing factor by several respondents.
Pharmacists also face challenges. At a hospital pharmacy in Chennai, a pharmacist named Kumar said he often receives questions from patients about why their insulin brand changed. “I have to explain that it's the same medicine, but patients don't believe me. They want to talk to the doctor,” he said. He added that the pharmacy sometimes runs out of the new brand during a transition, forcing patients to wait or return later. “It creates frustration for everyone.”
Policy Fixes That Could Stabilize Access
Recognizing the problem, Tamil Nadu's health department has begun piloting a more stable procurement model in two districts—Chennai and Madurai—starting in early 2026. Under the pilot, insulin contracts will be awarded for two years to the same manufacturer, with a clause allowing price renegotiation after one year. The goal is to give patients continuity while still benefiting from competitive pricing. “We want to balance cost and quality,” said Dr. S. Venkatesh, director of the Tamil Nadu Health Systems Project, who is overseeing the pilot.
Other policy fixes under discussion include incorporating therapeutic equivalence into tender criteria. Currently, tenders are awarded solely on price, with no consideration of whether the insulin is a pen or vial, or whether it is a human insulin or analog. Some experts argue that the state should specify a preferred device type (e.g., pre-filled pens) and require that the winning manufacturer supply it for the contract period. “Patients should not have to learn a new device every six months,” said Dr. Rajan. “If you want pens, pick one pen and stick with it.”
Another proposal is to allow exceptions for patients who are stable on a particular brand. Under a “continuity of care” clause, doctors could request that a patient continue receiving the same brand even if the tender changes, by sourcing it through a separate channel. However, this would require additional administrative work and could undermine the cost savings of bulk procurement. “We have to be careful not to create a two-tier system where some patients get better access than others,” Dr. Venkatesh said.
The pilot districts are also testing a transition period of three months when a brand change is unavoidable. During this window, the old and new insulins are both available, and patients are gradually switched under supervision. Early results from the first three months of the pilot show a reduction in dose-skipping and emergency visits, though the sample is small. “It's promising, but we need more data,” said Dr. Venkatesh. The state is also investing in patient education materials, with pictograms and local-language instructions, to accompany each switch.
In the Chennai pilot, preliminary data from the first quarter of 2026 show that only 8% of patients reported skipping doses after a brand change, compared to 15% before the pilot. Emergency visits for hyperglycemia dropped by about 10% in the pilot areas. However, the cost savings from the tender were slightly lower—around 25% instead of the previous 30–40%—because the longer contract period reduced competition. “We are still analyzing whether the health benefits justify the slightly higher procurement cost,” Dr. Venkatesh said. “The early signs are encouraging, but we need a full year of data.”
In Madurai, the pilot has faced challenges with manufacturer compliance. One supplier failed to deliver on time, leading to a temporary shortage. “We had to revert to the old system for a month,” said a local health official. The state is now considering penalties for non-delivery in future contracts.
Lessons for Other LMIC Public Insulin Programs
Tamil Nadu's experience offers cautionary lessons for other low- and middle-income countries that are expanding public insulin access through competitive tenders. Kenya's National Health Insurance Fund, for example, uses a similar tender system for essential medicines, including insulin, and has seen complaints from clinicians about frequent brand switches. In Bangladesh, a 2023 study found that patients in public hospitals faced brand changes every 4–6 months, leading to similar adherence problems. “The pattern is the same: cost savings upfront, but hidden costs in clinical outcomes and workforce strain,” said Dr. Anjali Singh, a health policy researcher at the Public Health Foundation of India.
The World Health Organization's prequalification program for insulin, launched in 2020, could help set stability standards. By certifying that certain brands are interchangeable, WHO could reduce the clinical risk of switching. However, the program is voluntary, and few manufacturers have sought prequalification for all their products. “Prequalification is a good start, but it doesn't solve the tender problem unless countries mandate that only prequalified insulins can be switched,” said Singh.
Global insulin price reduction initiatives, such as the one led by the Clinton Health Access Initiative, have focused on lowering prices through volume guarantees and pooled procurement. But as Tamil Nadu shows, price is not the only variable. “You can have the cheapest insulin in the world, but if patients can't use it consistently, it's not helping,” said Dr. Rajan. “We need to think about the whole supply chain, from procurement to patient education.”
The trade-offs are stark. A state that saves 30–40% on insulin costs may spend that money elsewhere—on emergency care for diabetic ketoacidosis, on complications from uncontrolled diabetes, or on clinician burnout. A modeling study by researchers at the Indian Institute of Technology Madras, published in early 2025, estimated that the net cost of frequent insulin switches could offset up to half of the procurement savings, once emergency visits and lost productivity are accounted for. “The savings are real, but they are not free,” said Dr. Rajan. Yet the pilot programs suggest that a middle ground may be possible: longer contracts, transition periods, and better patient education could reduce harm without eliminating savings entirely. The question is whether the state will scale these reforms statewide, or whether cost concerns will keep the system stuck in a cycle of cheap but disruptive supply.
For now, patients like Lakshmi and Murugan continue to navigate a system that prioritizes cost over continuity. Lakshmi said she has learned to ask for the same brand at each visit, but she knows that the next tender could change everything. “I just want my medicine to work,” she said. “I don't care if it's the cheapest or the most expensive. I just want it to be the same.”
This article is for informational purposes only and does not constitute personalized medical advice. Patients should consult their healthcare provider before making any changes to their insulin regimen.